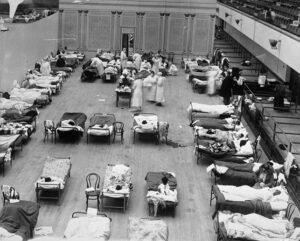
Imagine a doctor in the trenches of 1918, dealing not with the wounds of war, but with an unstoppable epidemic spreading rapidly among the soldiers. Field beds are filled with patients with high fevers, persistent coughs, and breathing difficulties. The medical staff, lacking effective treatment, battled an unknown virus that spread relentlessly, marking one of the most devastating influenza pandemics in history.
Between January 1918 and December 1920, the 1918 influenza pandemic – known as the “Spanish flu” – affected some 500 million people, or a third of the world’s population at the time. Estimates of the number of deaths vary between 20 and 100 million, making it one of the deadliest pandemics in recorded history. Its spread was facilitated by troop movements during the First World War, high urban population density and limited scientific understanding of influenza viruses.
This article does not simply recount a historical event but analyses its consequences and the lessons we can still learn from it. The 1918 pandemic was a turning point in the history of public health, highlighting the importance of prevention, scientific research, and international cooperation in managing health crises.
Today, thanks to advances in medicine, virology, and containment strategies, the world is better prepared than it was a century ago. However, understanding the past is essential to meeting future challenges. This article is based on historical and academic sources and should not be construed as medical or health advice.
_____________________
Recommended book: The Great Influenza: The Story of the Deadliest Pandemic in History 📖🦠💉 📖✨🌟 👉 Get it here! https://amzn.to/3DGAmg6 🔗💡 As an Amazon Associate, I earn a commission from qualifying purchases. This comes at no extra cost to you! ✅
_____________________
2. The origin of the pandemic
The exact geographical origin of the Spanish flu remains uncertain due to the lack of adequate historical and epidemiological data. However, several hypotheses have been formulated over time and the debate between historians and virologists is still ongoing. Some research suggests that the 1918 pandemic may have originated in the United States, with the first cases reported in January 1918 in Haskell County, Kansas. Here, local doctor Loring Miner noticed an unusually aggressive form of influenza and alerted the U.S. Public Health Service, but little attention was paid.
Another significant outbreak developed at Fort Riley, a US military installation, where cook Albert Gitchell fell ill on 4 March 1918, becoming the first recorded casualty. Within days, hundreds of men were infected, furthering the spread of the disease among American troops who were soon to be sent to Europe to fight in the First World War. The conditions in military camps and the constant movement of soldiers contributed to the rapid spread of the virus, making war the perfect vehicle for the for the transmission of the 1918 H1N1 virus.
Another accepted theory points to France as a possible first outbreak. The disease was named “La Grippe” in the French city of Rouen in April 1918, suggesting that the virus had been circulating in Europe for some time. Some researchers, such as Andrew Price-Smith, who has analyzed Austro-Hungarian archives, speculate that an epidemic broke out in Austria as early as 1917, while historian Mark Humphries has highlighted the possible role of the mobilization of Chinese workers called up to serve behind British and French lines during the war. Chinese documents from November 1917 report a respiratory epidemic in northern China, which some theorize may have traveled with workers to the European front. However, a 2016 report found no conclusive evidence of this direct transmission, suggesting that the virus was circulating in European armies before 1918.
The name ‘Spanish flu’ is actually misleading, as Spain was not the source of the pandemic. Unlike other countries involved in the conflict, Spain – which was neutral during the war – did not impose restrictions on the press. Spanish newspapers openly reported the spread of the disease, with alarming headlines even mentioning that King Alfonso XIII had been infected. In the belligerent countries, however, censorship restricted the dissemination of information to avoid panic among the population and troops. This media transparency led the world to wrongly associate Spain with the origin of the pandemic and contributed to the spread of the term “Spanish Flu”, which remains the most common name for the deadliest pandemic in modern history.
3. Global spread of the 1918 pandemic and historical impacts
Spanish flu spread around the world with astonishing speed, taking advantage of modern transport systems and the unprecedented mobility brought about by the First World War. Ships, trains, and the massive movement of troops acted as ideal vectors for the spread of the virus. Soldiers, often crowded together in precarious sanitary conditions, unknowingly carried the virus from front to front, spreading it rapidly across battlefields, military bases, and urban centers. The return of soldiers to their home countries exacerbated the health crisis and accelerated the transmission of the 1918 pandemic on a global scale.
The impact of the pandemic was devastating, affecting every continent and reshaping public health responses for future pandemics. In Europe, already exhausted by conflict, the disease spread rapidly among populations weakened by war and malnutrition, causing staggering mortality rates in towns and villages.
In the Americas, in both the United States and South America, the virus found fertile ground in rapid urbanization and a lack of adequate sanitation, resulting in a high death toll, with Brazil among the worst affected countries. In Asia, India suffered devastating human losses, with estimates of over 10 million deaths, while in China the flu spread widely, exacerbated by difficult living conditions in densely populated rural areas. In Africa, too, the pandemic reached remote areas, affecting populations already vulnerable to endemic diseases and healthcare shortages. Estimates of the total number of deaths vary between 20 and 100 million, making the Spanish flu one of the deadliest pandemics in recorded history. Although the Black Death in the 14th century killed a greater percentage of the world’s population at the time, the 1918 pandemic was deadlier in absolute terms.
Even compared to more recent health crises, such as the AIDS pandemic, which claimed fewer lives in 24 years than the Spanish pandemic did in just six months, the impact of the Spanish pandemic is extraordinary.
Even the 2009 influenza pandemic (H1N1), despite its global spread, resulted in significantly fewer deaths due to advances in epidemiological surveillance, vaccination, and available treatments. One of the most dramatic effects of the Spanish flu was the drastic reduction in life expectancy in the affected countries: in the United States, life expectancy is estimated to have fallen by around 12 years in the first year of the pandemic, an impact unprecedented in modern history.
4. Symptoms, progression, and stages of the disease
Typical symptoms of Spanish flu included a sudden onset of the disease, a pronounced feeling of general malaise with headache, muscle and back pain, fatigue, high fever (over 40 °C or 104°F), dry cough, and, in some cases, diarrhea and nausea. The heart rate could drop, and many patients experienced progressive difficulty breathing, which, in the most severe cases, rapidly developed into acute respiratory failure.
What made the 1918 pandemic so deadly was its ability to develop into fulminant pneumonia, either as a primary viral pneumonia or as a secondary bacterial pneumonia. The latter, favored by the weakened immune system, was the leading cause of death, usually killing by the eighth or ninth day after the onset of symptoms. In the most extreme cases, patients developed hemorrhagic fever and cyanosis, in which the skin turns bluish due to severe hypoxia.
The pandemic developed in several waves. The second wave, which began in late 1918, was significantly more lethal than the first. One possible explanation for its greater virulence is linked to the extreme conditions of the First World War. The virus circulated in crowded trenches, where natural selection may have favored the more aggressive strains. Soldiers with milder forms of the disease remained at the front, while the seriously ill were taken to overcrowded hospitals, spreading the virus to the rear.
A particularly puzzling aspect of the Spanish flu was the high mortality among healthy young adults, especially in the 20-40 age group. This was unusual because seasonal flu usually affects children and the elderly, the most vulnerable groups. Several theories have been put forward to explain this phenomenon. Some researchers speculate that the virus had a particularly aggressive mutation and that the immune system of young adults overreacted in an excessive and lethal way, triggering a storm of cytokines, i.e. an uncontrolled inflammatory response, which ended up severely damaging the lungs. Other researchers suggest that environmental and climatic conditions made the population more susceptible to infection, while another hypothesis links the different immune responses to childhood exposure to earlier strains of the virus.
In the absence of specific treatments and effective antiviral therapies, the measures taken to control the spread of the pandemic were essentially containment. Health authorities encouraged the use of masks to limit the transmission of the virus, while strict quarantines were imposed to isolate the sick and contain the spread of infection. Schools, churches, theatres, and public places were closed in many cities, a rudimentary lockdown that anticipated measures taken in modern pandemics. The population was urged to observe rules of personal hygiene and social distancing, but in the absence of in-depth virological knowledge, many resorted to improvised and often ineffective remedies. Among these, experimental vaccines based on the Pfeiffer bacillus, mistakenly thought to cause influenza, proved useless. In some cases, the proposed treatments made things worse: the massive use of aspirin in potentially toxic doses, for example, may have contributed to increased mortality by causing accidental poisoning and pulmonary complications in already weakened patients.

5. The medical and social response
The role of doctors and scientists during the Spanish flu was severely limited by the medical knowledge of the time and the lack of advanced diagnostic tools. The influenza virus had not yet been identified and was not discovered until 1933, more than a decade after the end of the pandemic. Initially, many experts mistakenly believed that influenza was caused by a bacterial infection caused by Pfeiffer’s bacillus (Haemophilus influenzae). This belief led to the testing of vaccines based on this bacterium, which proved completely ineffective in controlling the spread of the disease. Without a real understanding of the pathogen, doctors could only offer palliative care, trying to alleviate symptoms rather than stopping the virus at its source.

The strategies adopted by different countries to combat the 1918 pandemic were different but had many similarities in that they were non-pharmaceutical interventions. Quarantine and isolation of the sick were widespread measures, although challenging to apply on a large scale, especially in crowded cities. In many urban areas, schools, businesses, and entertainment venues were closed to reduce social contact and slow the transmission of the virus. Some governments imposed restrictions on public transport and banned gatherings in the hope of limiting the spread of influenza in the most affected communities. In parallel, public information campaigns were launched to promote personal hygiene, encouraging the use of tissues and masks to reduce the risk of infection.
Even in 1918, misinformation and false reports played a significant role in complicating the management of the pandemic. The lack of a clear understanding of the disease and the high mortality rate contributed to the spread of misconceptions that fuelled fear and superstition. Some unsubstantiated theories suggested that the disease was caused by poisonous gases used in warfare, while others attributed its spread to atmospheric changes or divine retribution. Remedies with no scientific basis, such as herbal concoctions, alcohol, and improvised drugs, were promoted by charlatans and profiteers, adding to the confusion of the population. With no central coordination and often conflicting information, the response to the pandemic was fragmented and, in many cases, ineffective in containing the growing number of victims.

6. The legacy of the pandemic
The Spanish flu left an indelible mark on public health and scientific research and had a profound impact on future pandemic prevention and response strategies. Its devastating scale highlighted the need for more effective global health surveillance systems capable of detecting and monitoring the emergence of new infectious diseases in a timely manner. It also highlighted the importance of increased investment in virology research, the development of vaccines and antiviral therapies, and the establishment of pandemic preparedness plans to ensure rapid and effective responses to potential health crises.
The lessons learned from the 1918 pandemic have been crucial in addressing subsequent public health challenges, including the COVID-19 pandemic. Many of the measures taken between 2020 and 2023, such as the use of masks, social distancing, and quarantine, echo strategies implemented a century earlier. However, the speed of vaccine development and current scientific knowledge represent significant advances over 1918, when understanding of viruses was in its infancy, and there were no specific treatments for influenza.
Despite its enormous scale and devastating impact, the Spanish flu has long been forgotten in the collective memory. Several factors contributed to this kind of historical amnesia. The coincidence with the First World War, which monopolized public and government attention, reduced awareness of the pandemic’s actual severity. In addition, the relatively rapid decline of influenza between 1919 and 1920 led the world to try to turn the page and focus on post-war reconstruction, leaving the suffering caused by the virus in the shadows. In part, there may also have been a collective reluctance to remember such a traumatic event, a common phenomenon in large-scale public health tragedies. Only in recent years, particularly after the COVID-19 pandemic, has there been a renewed historical interest in the 1918 pandemic, with in-depth studies providing a better understanding of its dynamics and the importance of its lessons for the future of global health.
7. Conclusion
The 1918 influenza pandemic is a seminal chapter in public health history and provides important lessons in the management of public health emergencies. It demonstrated how quickly a virus could spread on a global scale and highlighted the need for effective preparedness to deal with future epidemiological crises.
Lessons learned from this pandemic have contributed to the development of containment strategies, the promotion of scientific research, and the strengthening of international health cooperation. Understanding the past allows us to avoid past mistakes and improve our ability to respond to emerging public health threats.
Thanks to advances in virology, surveillance systems, and medical technology, the world now has more advanced tools than it did a century ago. However, prevention remains the most effective strategy for reducing the impact of pandemics. Investment in research, vaccine development, and evidence-based public health policy is key to protecting future generations.
Studying the history of the 1918 pandemic is not just an academic exercise but an opportunity to strengthen global resilience and promote concrete action to protect public health. Only through informed preparation and effective international cooperation can we successfully meet the health challenges of the future.
_____________________
Curious to see these medical stories come to life? Visit my YouTube channel, where I’ve turned these stories into compelling documentaries. 👉 Click this link to explore the channel! 🔗💡
_____________________
Short Bibliography
Andrew T. Price-Smith, Contagion and Chaos. Disease, Ecology and National Security in the Era of Globalization, 2009.
Howard Phillips, The re-appearing shadow of 1918: trends in the historiography of the 1918–19 influenza pandemic, in Can Bull Med Hist, vol. 21, n. 1, 2010, pp. 121-134.
Niall Johnson and Juergen Mueller. “Updating the Accounts: Global Mortality of the 1918-1920 “Spanish” Influenza Pandemic.” Bulletin of the History of Medicine 76, no. 1 (2002): 105-115.
Mark Humphries. Paths of Infection: The First World War and the Origins of the 1918 Influenza Pandemic. War in History, 21(1), 2014, 55-81.
Related Links:
https://www.paho.org/en/who-we-are/history-paho/purple-death-great-flu-1918
https://pubmed.ncbi.nlm.nih.gov/35661699/
Disclaimer
The content on the blog “Medical History Book” is for informational and entertainment purposes only. It is not intended to provide medical advice, diagnosis, or treatment. Readers should not rely on the information provided in the articles for medical decisions. Always consult a qualified healthcare professional for any medical concerns or questions. The authors and creators of this blog are not responsible for any actions taken based on the information provided herein. Use this blog at your own discretion.